Overview
Pronation describes a slight inward rolling motion the foot makes during a normal walking or running stride. The foot (and ankle) roles slightly inward to accommodate movement. Some people, however, over-pronate and roll more than normal. With over-pronation, the arch of the foot flattens and causes excessive stress and pressure on the soft tissues of the foot. Over-pronation is more common in those with flat feet, and can lead to foot aches and pain, such as plantar fasciitis, Shin Splints and Knee Pain.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
Pronation describes a slight inward rolling motion the foot makes during a normal walking or running stride. The foot (and ankle) roles slightly inward to accommodate movement. Some people, however, over-pronate and roll more than normal. With over-pronation, the arch of the foot flattens and causes excessive stress and pressure on the soft tissues of the foot. Over-pronation is more common in those with flat feet, and can lead to foot aches and pain, such as plantar fasciitis, Shin Splints and Knee Pain.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
 Even though bunions are a common foot condition, they are probably the one with the most misconceptions. Many people suffer unnecessarily with the pain of bunions for years before seeking treatment out of fear about the ?surgery?. The good news is that most bunion pain can be resolved without surgery.
Even though bunions are a common foot condition, they are probably the one with the most misconceptions. Many people suffer unnecessarily with the pain of bunions for years before seeking treatment out of fear about the ?surgery?. The good news is that most bunion pain can be resolved without surgery.
 The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon.
The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon.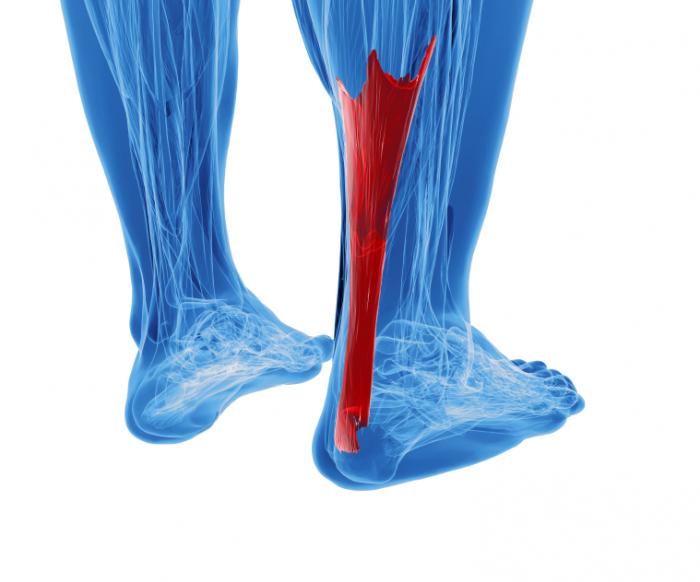






 RSS Feed
RSS Feed
